How Do You Know If Your Migraines Are Chronic? What the Number Actually Means
For a long time, I had no idea there were two different categories of migraine. I knew I got them often. I knew they disrupted my life. But it was not until I finally went to my doctor looking for real help that I had to do something I had never done before: count them.
When I counted, the number stopped me cold.
That moment, sitting in a doctor's appointment putting a real number against something I had been quietly managing for years, is how most people find out their migraines are chronic. Not through a formal test. Not through some defining attack. Through counting, and realizing the total is much higher than they thought.
If you are reading this because you suspect your migraines are more frequent than "normal," this post is for you. Here is what chronic migraine actually means, how it gets diagnosed, what the signs are that most people miss, and what life at 15+ days a month honestly costs.
What Is Chronic Migraine?
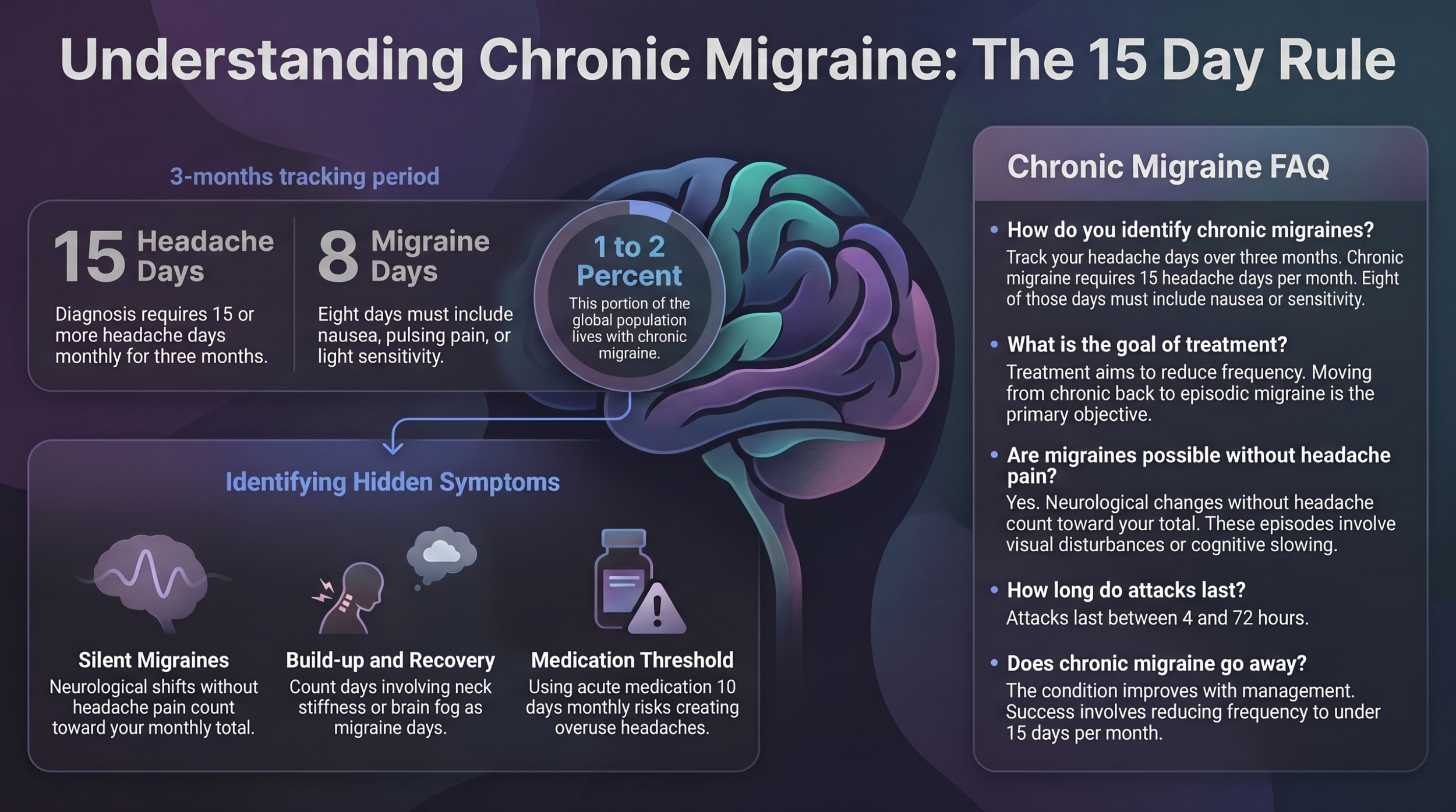
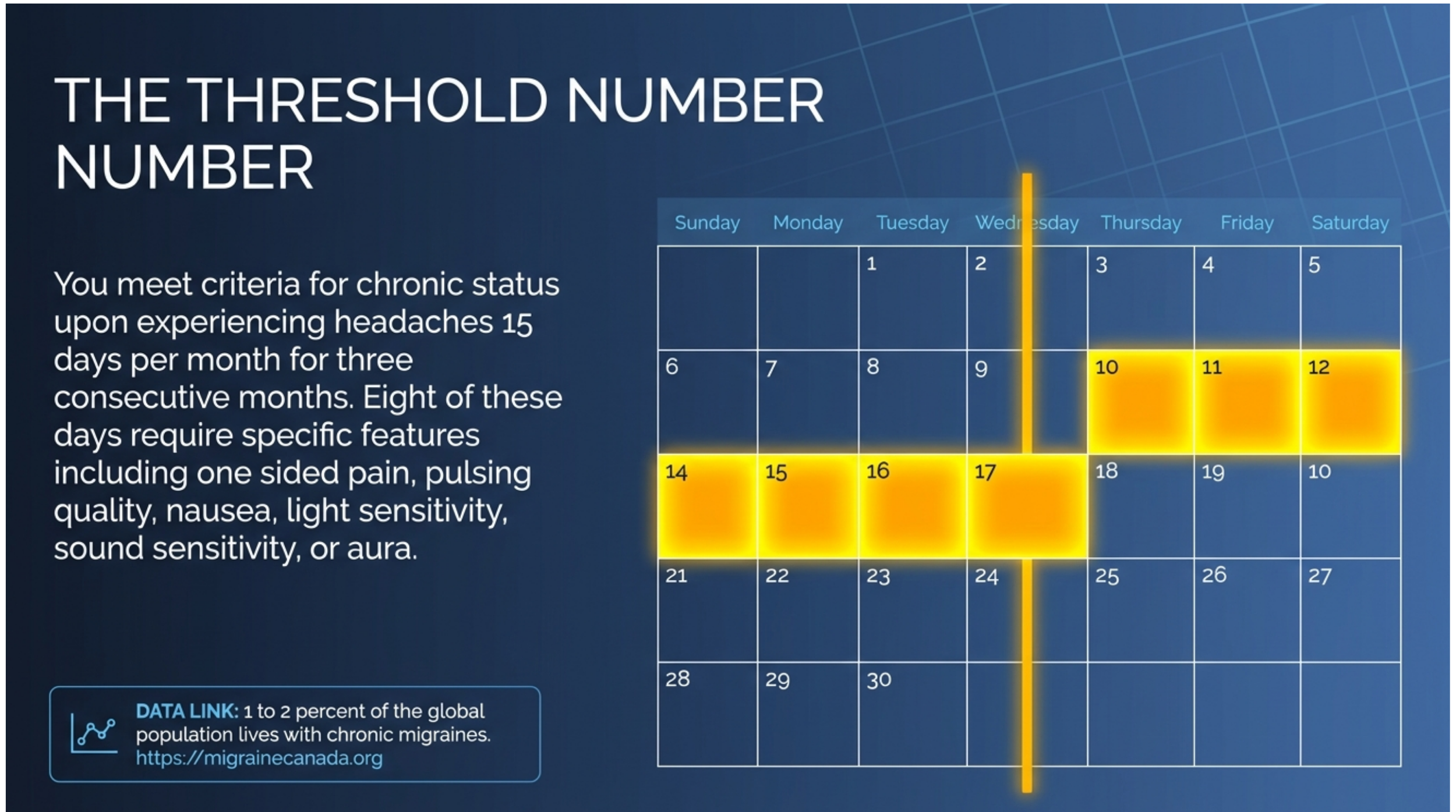
Chronic migraine is a specific clinical classification. According to the International Classification of Headache Disorders (ICHD-3), you meet the criteria for chronic migraine when you experience headaches or migraines on 15 or more days per month, for more than three months, with at least 8 of those days having migraine features specifically.
The days that count do not all have to be severe, full migraine attacks. Tension-type headache days count toward that 15-day threshold too. What separates chronic migraine from a general headache problem is those 8 days per month carrying migraine-specific features: one-sided pain, pulsing quality, nausea, light sensitivity, sound sensitivity, or aura.
Migraine Canada estimates that around 1-2% of the global population lives with chronic migraine. It is far less common than episodic migraine and significantly more disruptive.
The Difference Between Episodic and Chronic Migraine
Episodic migraine means fewer than 15 headache days per month. That is the line. Under 15 days is episodic. At or above 15 days for three consecutive months is chronic.
This distinction matters for two reasons. First, the treatment approach differs. Preventive medication becomes a higher priority at the chronic level because the frequency is too high to manage with acute treatment alone. Second, and this is the thing most clinical articles skip over entirely, the goal of treatment changes.
When you have chronic migraine, you are not trying to eliminate migraines. You are trying to get back to episodic. Fewer than 15 days a month. That is the realistic target, and it is a meaningful one. It took me time to accept that framing, but it is more honest and more achievable than chasing a cure.
I have gotten there. Four months at a stretch before something shifts, a bad weather season, a high-stress period at work, and the frequency climbs back up. Getting back to episodic is possible. Staying there permanently is harder. But knowing it is achievable is what keeps the management work worth doing.
The Signs Most People Miss
You Are Counting the Wrong Days
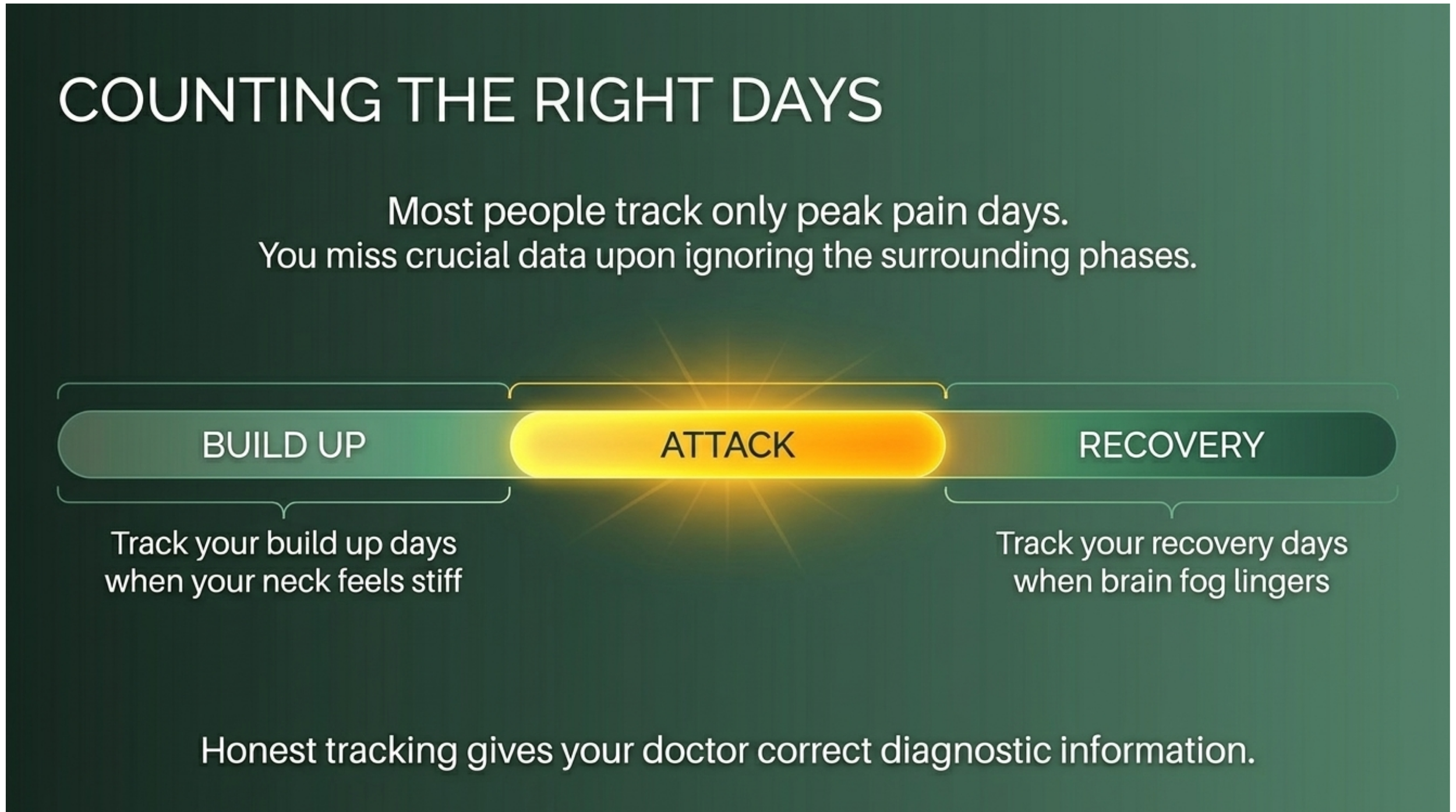
Most people count the days when the headache pain peaks. The days they had to lie down, cancel plans, or call in sick. Those are the obvious migraine days, and they are important. But they are not the whole picture.
When your migraines are chronic, you spend a significant amount of time in build-up or recovery that does not get counted. The day before a bad attack, when your neck is stiff, and your appetite is off, and you feel slightly wrong but cannot name it. The day after, when the pain is gone, but the fog has not lifted, and everything still costs more than it should.
When I am not in an active attack, I am often in one of those two states. Either something is building, or I am coming down from something. There is rarely a clean break in between. That is the part of chronic migraine that does not show up in a symptom list, and it is the part that makes 15 days a month feel like more.
If you are tracking your migraine days honestly, count the build-up days that stop you from functioning normally. Count the recovery days that take half your capacity. The number you end up with is probably closer to the truth than the one you started with.
Silent Migraines Count Too
This is the detail that more than doubled my recorded migraine count when I finally understood it.
For years, I had days where something was clearly wrong. I was not having headache pain, so I did not classify them as migraines. But I felt off in a way that was not a cold, not anxiety, not tiredness. I did not know what to call it or how to manage it, which meant I was not managing it at all.
It was during a follow-up call with my doctor, when I was describing these episodes, that we worked it out together. What I was describing was migraine without headache, also called silent migraine or migraine aura without headache. It is a real migraine type, it carries all the neurological features of a migraine, and it counts toward your monthly total.
Having a name for it was a significant relief. When something has a label, you know how to treat it. When it does not, you are left guessing every time it happens. If you have days where something feels neurologically off, where your vision shifts, your thinking slows, or a familiar wrongness settles in without a headache following, talk to your doctor about whether silent migraines are part of your picture. You can read more about the low-grade migraine experience, including what silent migraines feel like from the inside.
How Chronic Migraine Is Diagnosed
What the Diagnostic Criteria Actually Mean
Your doctor will often look at your headache history over at least three months. They will ask
How many days per month do you experience any headaches?
How many of those carry migraine-specific features?
What does your current acute medication use look like?
Do you have a personal or family history of migraine?
There is no imaging test or blood test that diagnoses chronic migraine. The diagnosis is clinical, meaning it is built from your reported history. This is why counting accurately matters. A migraine diary, even a basic one, gives your doctor the information they need to classify what you are dealing with and make a treatment plan that actually fits the frequency.
What If My Frequency Changes Month to Month?
It does for most people. Chronic migraine is not a fixed state. It fluctuates with triggers, seasons, stress levels, and how well your prevention is working.
The diagnostic threshold of three months is there to separate chronic migraine from a temporary high-frequency period. A bad month after a stressful event does not automatically mean you have chronic migraine. But if your frequency has been consistently elevated across multiple months, even with variation, that pattern is worth discussing with your doctor.
Seasonal triggers in particular, weather shifts in spring and fall, high humidity in summer, and pressure changes before storms, can push someone from episodic into chronic territory for months at a time. You can read more about how weather affects migraine frequency in this post: Weather and Migraines: Why Barometric Pressure Triggers Attacks.
What Living at 15 Days a Month Actually Costs
This is the section that does not exist in any clinical article, and it is the part I most want to share.
Living with chronic migraine is exhausting in a way that is physical, mental, and emotional all at once. You are not just dealing with the attacks themselves. You are managing the anticipation of the next one, the recovery from the last one, and every normal responsibility in between.
Life does not pause because your head hurts. The bills still come. The work still needs doing. The groceries still need to be bought. When you live alone and manage this without a support system at home, you carry all of it yourself, through every phase of the cycle.
There is no real break. You are either in a build-up, in an attack, in a recovery, or in a brief window of feeling something close to normal, and part of your brain is already watching for the next sign. That constant vigilance is its own kind of tired.
The emotional cost is real too. The guilt of canceled plans, the frustration of knowing what you need to do to manage your condition and still not always being able to do it, the grief of losing days you cannot get back. These are not weaknesses. They are the honest costs of a neurological condition that does not give you days off.
If you recognize this exhaustion, you can read more about the emotional side in this post.
Treatment Goals and What to Expect
The goal of treatment for chronic migraine is to reduce the frequency and severity of attacks. Getting from chronic back to episodic. Your treatment plan will likely include a combination of preventive approaches and acute options.
Preventive treatments are taken daily or regularly, regardless of whether you have a migraine that day. They include medications prescribed by your neurologist, as well as evidence-based supplements like magnesium, riboflavin (B2), and CoQ10, which are best discussed with your doctor before starting. Lifestyle factors, protecting sleep, managing stress, keeping meals consistent, and tracking triggers, are also part of prevention at the chronic level.
Acute treatments are what you reach for during an attack to reduce its severity and duration. This is where things get more complicated.
A Note on Medication Overuse
If you take acute medication frequently, this is a calculation you are probably already making, even if you have not named it.
According to the ICHD-3 criteria, using certain acute medications on 10 or more days per month can lead to medication overuse headache, a condition where the medication itself begins to contribute to headache frequency. For triptans and combination analgesics, that threshold is 10 days per month. For simple pain relievers like acetaminophen or NSAIDs, it is 15 days.
I think about this every time I consider taking medication. Is this the right moment, or should I try something else first? Is the attack building to a point where waiting will cost me more? The timing question is always hard to answer, and it is one of the harder parts of managing chronic migraine on a day-to-day basis. Your doctor or neurologist is the right person to help you build a protocol that accounts for your specific frequency and medication type.
You can find more details on the first-30-minutes home management approach in this post: Finding Migraine Relief at Home.
Chronic Migraine FAQs
-
The clinical threshold is 15 or more headache or migraine days per month for at least three months, with at least 8 of those days carrying migraine features. If you are close to that number and have been for several months, talk to your doctor. Tracking your days accurately, including low-grade days and recovery days, gives you and your doctor the clearest picture.
-
Episodic migraine means fewer than 15 headache days per month. Chronic migraine means 15 or more days per month across at least three months. The treatment approach differs significantly at the chronic level, with preventive medication becoming a higher priority.
-
No, but it can improve. The goal of treatment is getting frequency back down to episodic levels, under 15 days per month. Some people achieve this and maintain it long-term. For others, including me, it is a moving target that improves significantly with the right management but can climb again during high-trigger periods. Getting to episodic is achievable. Staying there permanently depends on many factors outside your control.
-
Individual attacks vary. A single migraine can last anywhere from 4 to 72 hours, according to the Cleveland Clinic. At the chronic level, what changes is not the length of individual attacks but the frequency of them, meaning there is much less time between cycles.
-
Yes. Migraine without headache, also called silent migraine or migraine aura without headache, is a recognized migraine type. It includes neurological symptoms like visual disturbances, cognitive slowing, or sensory changes without the headache phase. These episodes count toward your monthly migraine total.
-
The most effective approach combines preventive treatment, acute treatment used carefully within safe frequency limits, lifestyle factors like consistent sleep and meals, and accurate tracking to identify your personal triggers. Talk to your neurologist about a plan that fits your specific frequency and migraine type.
The content on this page is based on personal experience and is not medical advice. Always consult your doctor regarding your migraine management and treatment plan.
QUICK ANSWER: Chronic migraine means having a headache or migraine on 15 or more days per month, for at least three months, with at least 8 of those days carrying migraine features. Most people do not know they are in chronic territory until they sit down with a doctor and put an actual number to it. Silent migraines, the ones without a headache, count toward that total and are frequently missed entirely.