My Dentist Found TMJ. My Migraines Had Questions.
I was sitting in the dentist's chair when they mentioned, almost in passing, that my jaw clicks. And offhandedly said it was likely TMJ disorder, and asked if it was causing me any pain… when I said it wasn’t, they said then there was no treatment needed at this point. Reasonable advice. I nodded, went home, and then did what I always do when a new potential medical issue enters the picture.
I started researching.
Because here is the thing about living with chronic migraines: you learn to pay attention to every variable. And jaw tension has been part of my prodrome for as long as I can remember. I just never had a name for it.
What Is TMJ Disorder?
The temporomandibular joint is the hinge that connects your lower jaw to your skull. You have one on each side of your face, and they work together with the surrounding muscles and tissues every time you chew, speak, or yawn.
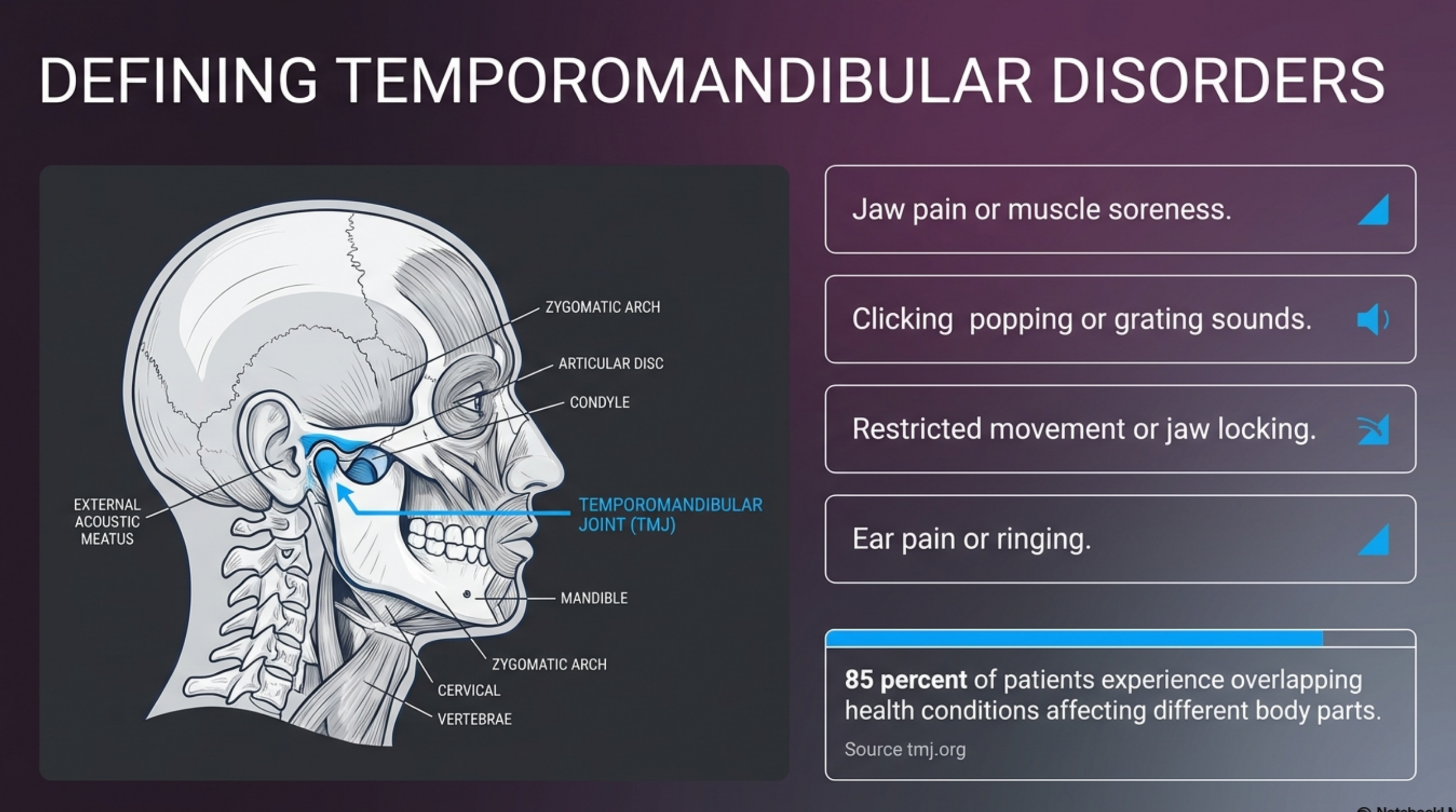
Temporomandibular disorders (TMDs) are a group of conditions that affect these joints, the muscles around them, or both. According to the National Institute of Dental and Craniofacial Research, there are three main categories:
Disorders of the joints themselves
Disorders of the chewing muscles
Headaches associated with TMD
Symptoms vary widely between people. Some experience significant pain. Others, like me, have a clicking jaw with no pain at all. Common symptoms include:
Jaw pain or muscle soreness
Clicking, popping, or grating sounds when moving the jaw
Difficulty opening or moving the jaw fully
Jaw locking
Ear pain, fullness, or ringing
Neck and shoulder pain
Headaches
Research from the TMJ Association shows that approximately 85% of people with TMD also experience other health conditions affecting different parts of the body, including headaches, sleep disturbances, fibromyalgia, and irritable bowel syndrome. TMD rarely shows up alone.
The Connection Between TMJ Disorder and Migraines
This is the part that sent me down a research spiral at 10pm on a Tuesday.
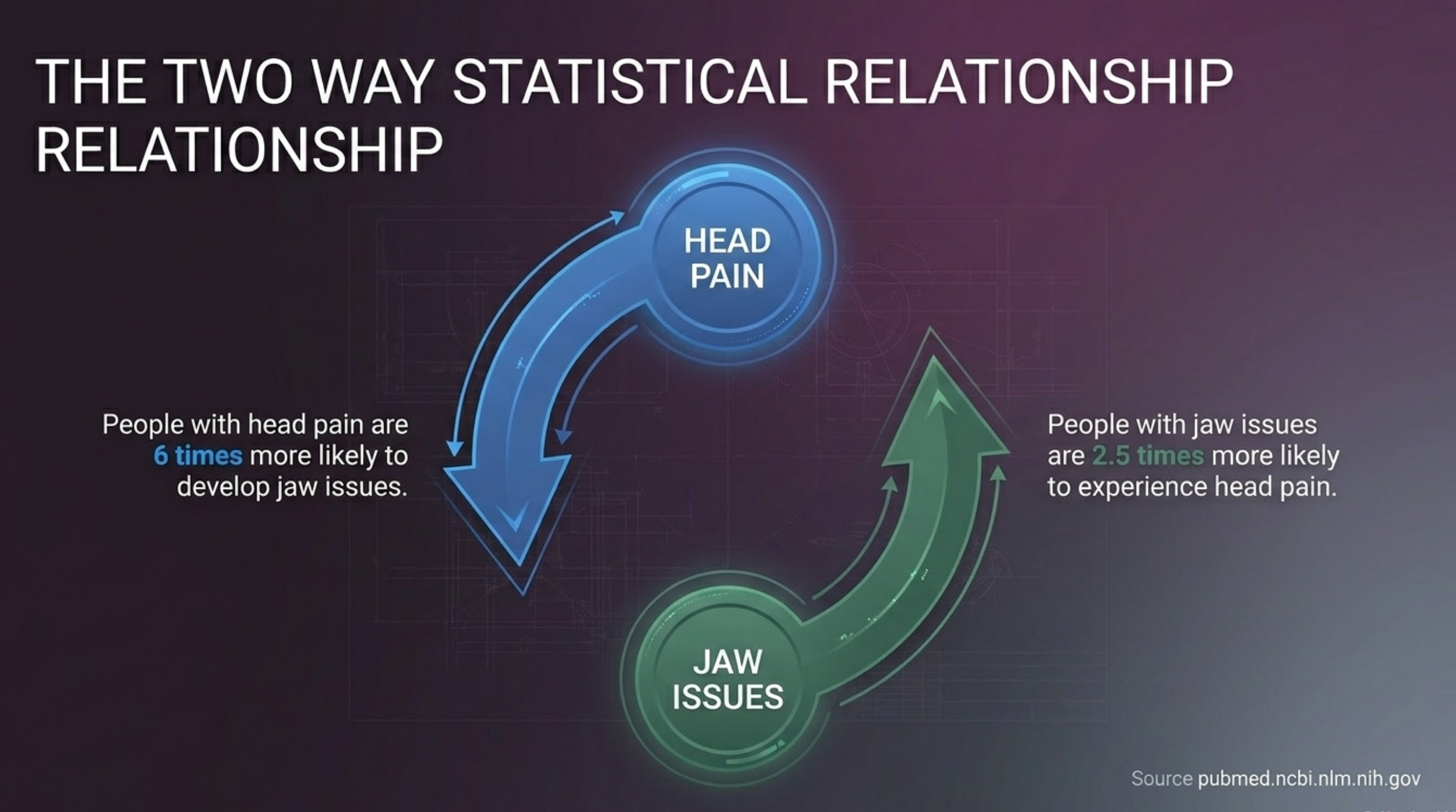
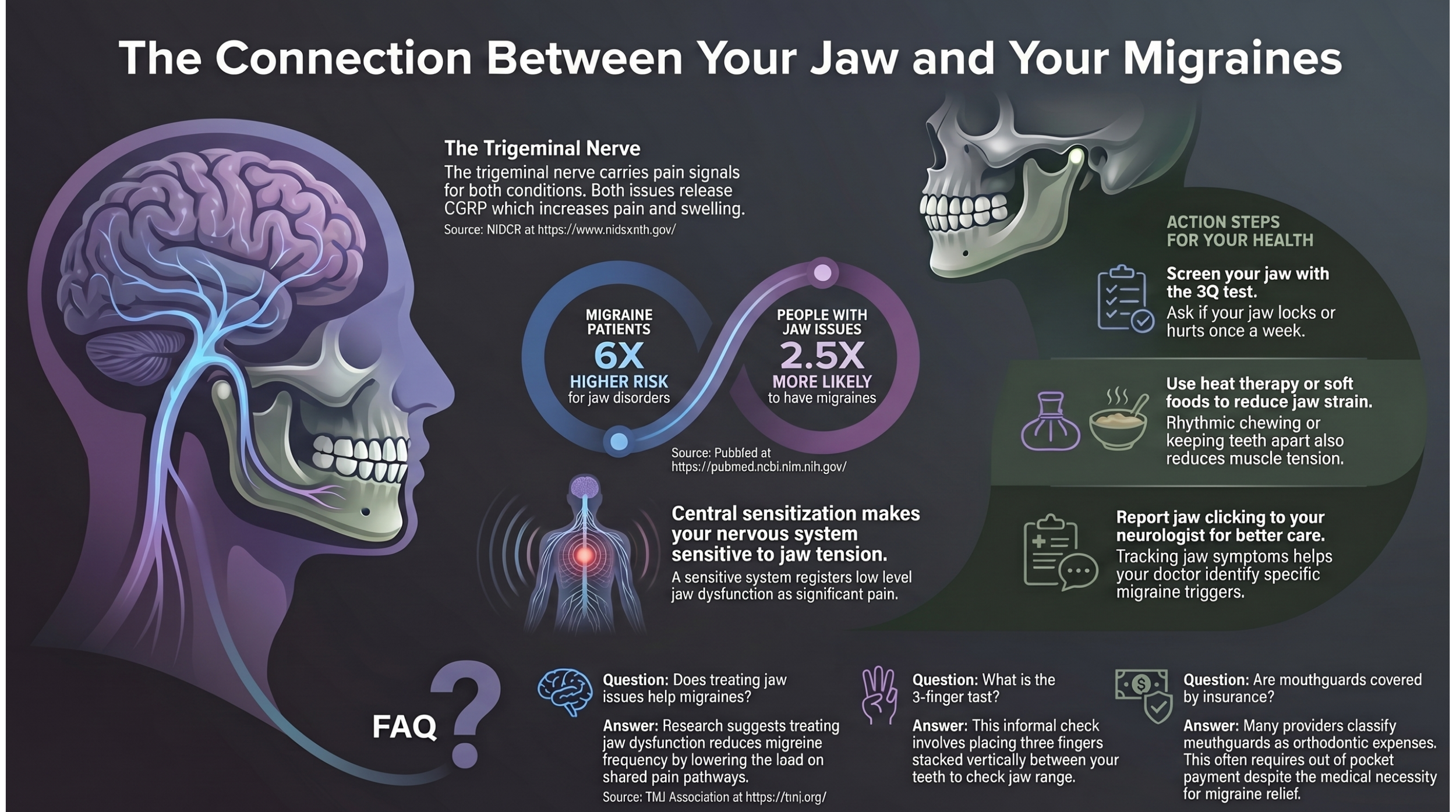
TMD and migraines have what researchers call a bidirectional relationship. That means having one condition meaningfully increases your risk of developing the other. A study published in PubMed found that people with migraines were about six times more likely to develop TMD, and people with TMD were about 2.5 times more likely to have migraines. Treating one condition effectively may reduce the severity or frequency of the other.
Why are they so connected? Several mechanisms appear to be involved.
The Trigeminal Nerve
The trigeminal nerve is the main pain pathway that carries sensation from your face, jaw, and head to your brain. During a migraine attack, this nerve becomes activated, which produces the head and facial pain associated with migraines. Because the trigeminal nerve also carries sensation from the jaw joint and surrounding muscles, dysfunction in that area can feed directly into the same pain system. When your jaw is tense or inflamed, it is sending signals through the same highway your migraines travel.
CGRP: The Connecting Thread
During a migraine attack, the trigeminal nerve releases a substance called CGRP (calcitonin gene-related peptide), which increases pain, causes swelling, and widens blood vessels. Research published in the journal Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology found that people with TMJ pain have elevated levels of CGRP in the jaw area. People with migraines also show elevated CGRP levels during and between attacks. The same inflammatory process appears to be at work in both conditions.
Central Sensitization
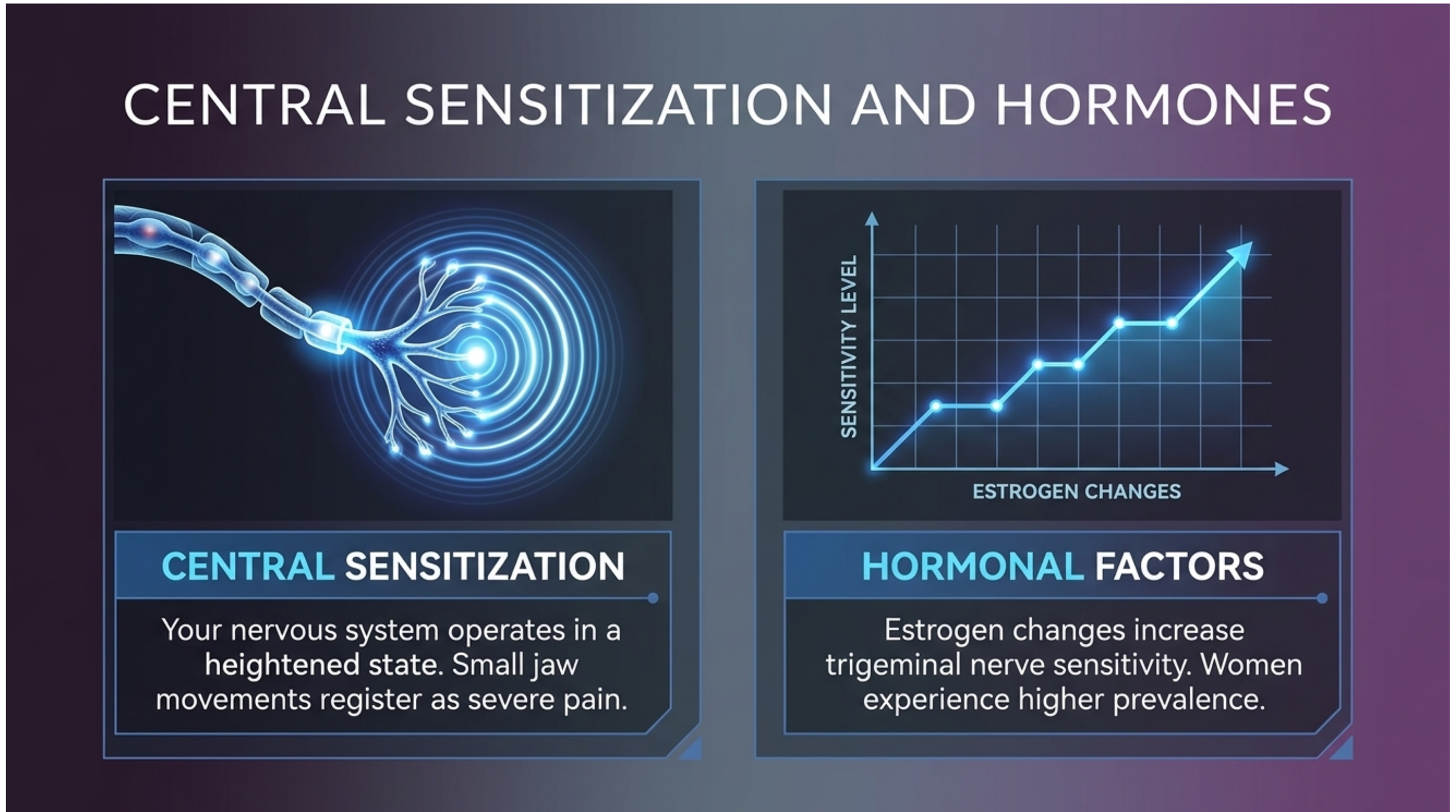
Central sensitization occurs when the nervous system becomes more sensitive over time, making pain signals feel stronger than they normally would. For people with chronic migraines, the nervous system is already operating in a heightened state. This makes it easier for jaw tension or TMD-related dysfunction to register as pain or to tip an attack over the threshold. If you have been managing migraines for years, your system is already primed.
Hormonal Factors
Both TMD and migraines are significantly more common in women. Changes in estrogen levels increase sensitivity in the trigeminal nerve, which helps explain why both conditions peak during reproductive years and often shift around hormonal changes like pregnancy or perimenopause.
Jaw Tension as a Migraine Trigger: The Glass Filling Quietly
If you have read my post on the migraine threshold, you know I think about my triggers as pebbles and rocks dropping into a glass of water. When the glass overflows, a migraine begins. The question is always: what filled it?
For years, I tracked the obvious ones. Weather, stress, skipped meals, allergy season. But jaw tension? That one was invisible to me. I knew it was there. I felt it in my prodrome, that throbbing tightness in my jaw and teeth, always on the same side as the migraine that followed. I just never connected it to a structural reason.
Now I am wondering how many times my glass was being pre-filled by a jaw joint I did not know was doing anything unusual.
The frustrating part is that even with this knowledge, I am not able to do much about it. My TMJ does not cause me pain on its own, so it does not meet the threshold for treatment. But for those of us with chronic migraines, a trigger does not need to hurt independently to be quietly contributing to the pattern. It just needs to add weight to the glass.
The Cost Reality Nobody Talks About
This is the part of the conversation that tends to get left out of clinical articles, so I am going to say it plainly.
Even with extended health and dental coverage through work, my coverage only goes to 80% of eligible expenses. And the word eligible is doing a lot of work in that sentence.
My mouthguard, which is one of the most common first-line tools for managing jaw tension and TMD, was classified as an orthodontic expense by my insurance provider. Orthodontic coverage is a separate category with its own annual maximum, and I had to pay for it largely out of pocket. It is not a luxury item. It is a piece of equipment that prevents me from clenching my teeth, which is directly relevant to both my jaw health and my migraines. But the classification system does not care about that connection.
Migraine medications in Canada are not covered under provincial health plans in most cases. Without private insurance, the costs can add up quickly. Even with coverage, co-pays on specialty medications quickly add up. For many people managing chronic migraines, every new potential avenue for treatment comes with a cost calculation attached.
The research suggests that treating TMD can reduce migraine frequency. That is a meaningful finding. But it lands differently when you are already budgeting across medications, supplements, acupuncture, and other tools your insurance covers partially or not at all. Adding dental specialist visits, intraoral appliances, or other TMD-specific treatments is not a simple decision for most people navigating this on a fixed income.
I raise this not to complain, but because I know I am not the only one doing this math.
How to Know If Your Jaw Is Part of Your Migraine Pattern
One of the things I have learned over ten years is that identifying where a migraine is starting changes how I manage it. A migraine that originates in the neck or base of the skull responds differently from one that starts behind the eye or in the jaw and tooth area.
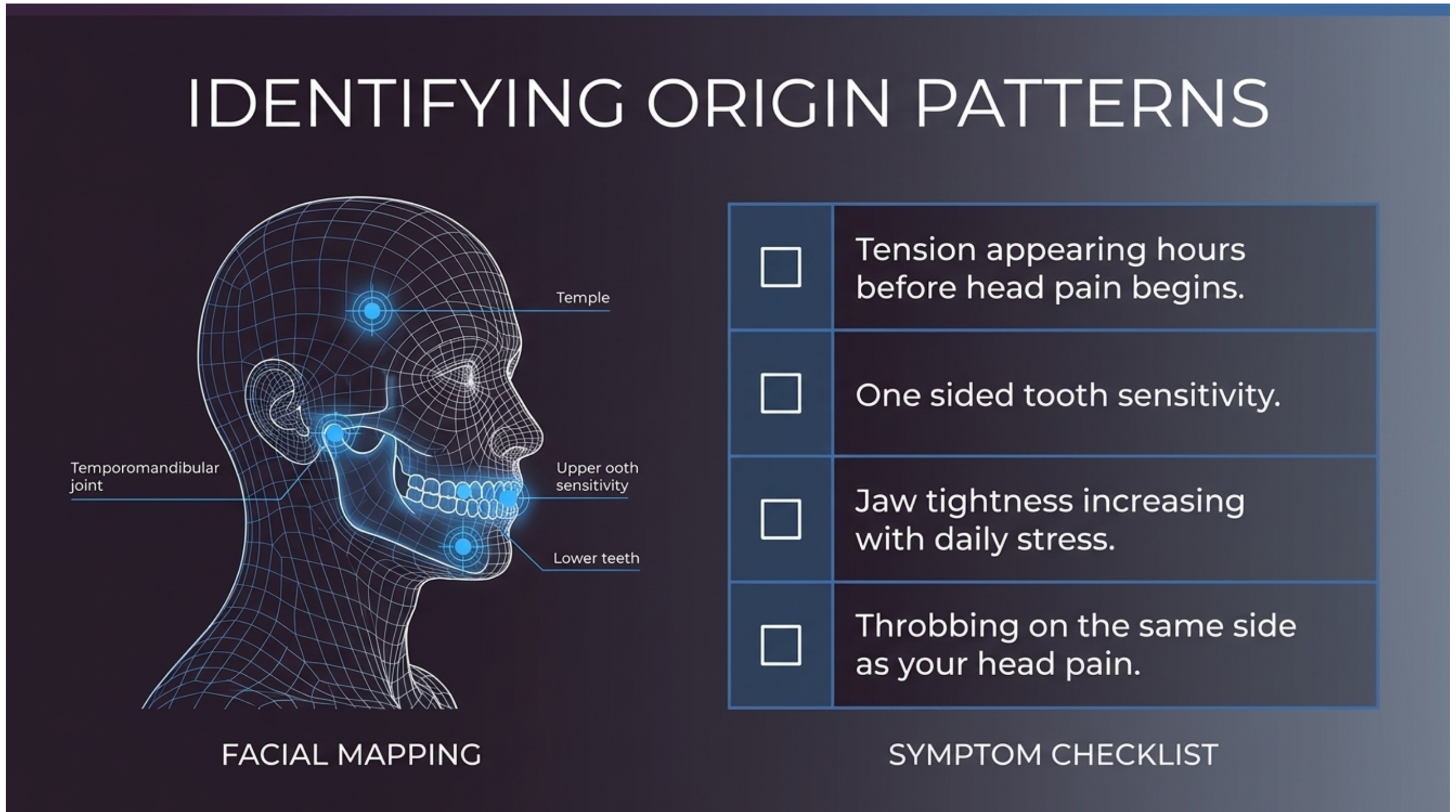
For jaw-origin migraines specifically, here is what I watch for:
Tension or throbbing in the jaw that appears hours before head pain
Tooth sensitivity or aching on one side, usually the same side as the migraine
Jaw tightness that worsens with stress or when I am not consciously relaxing my face
The sensation being one-sided rather than generalised
My main tool for jaw-tension migraines when they first develop is chewing gum. It sounds simple, but there is a mechanical logic to it. The act of rhythmic chewing engages and then releases the jaw muscles, which can help interrupt the tension cycle. It is not a fix, but it is part of my first-response toolkit when I feel jaw tension building as part of a prodrome.
If you notice a similar pattern, it is worth tracking which side your jaw tension appears on and whether it correlates with which side your migraines favour. That kind of detail is useful information for your doctor.
TMD Diagnosis and Treatment Options
If you suspect jaw dysfunction is part of your migraine picture, here is what the assessment and treatment landscape looks like.
Screening
One commonly used screening tool is the 3Q/TMD, a set of three yes-or-no questions:
Do you have pain in your temple, face, jaw, or jaw joint once a week or more?
Do you have pain once a week or more when you open your mouth or chew?
Does your jaw lock or become stuck once a week or more?
A positive answer to any of these suggests that further evaluation by a healthcare provider may be worthwhile. Your general dentist is typically the right first point of contact for suspected TMD.
Conservative first-line treatments
The National Institute of Dental and Craniofacial Research recommends starting with the safest, reversible options. Surgery is considered in only about 5 to 10% of cases and only after all conservative approaches have been tried.
Conservative options often include:
Soft foods to reduce jaw strain
Heat or cold therapy applied to the jaw
Avoiding wide yawning, extended gum chewing, or other high-strain movements
Keeping teeth slightly apart when not actively eating or speaking
Stress management, since jaw clenching and grinding increase under stress
Physical therapy
Intraoral appliances (mouthguards), used only during sleep and for short-term periods to avoid permanent bite changes
Cognitive behavioural therapy for pain management
Medications
Some medications overlap between TMD and migraine treatment. Short-term NSAIDs like ibuprofen can address jaw pain temporarily. Amitriptyline, a tricyclic antidepressant, has evidence for both chronic pain and migraine prevention. OnabotulinumtoxinA is FDA-approved for chronic migraine and used off-label for TMD-related pain, though evidence for the latter remains mixed.
It is important to note that none of these medications are FDA-approved specifically for TMD. Any treatment decisions should involve your neurologist and your dentist or orofacial pain specialist working together.
What This Means If You Already Have Chronic Migraines
If you are already managing chronic migraines, the TMD connection is worth taking seriously for a few reasons.
Central sensitization means your nervous system is already operating at a higher baseline sensitivity. Jaw dysfunction does not need to be severe to contribute to your migraine pattern. A low-level, asymptomatic TMJ issue, one that causes no independent pain, could still be adding to the cumulative load that tips you into an attack.
The bidirectional relationship also means that effectively managing one condition may reduce the burden of the other. If jaw tension is a consistent part of your prodrome, reducing that tension through conservative measures could reduce the frequency of attacks it contributes to.
Both conditions disproportionately affect women, and both are influenced by hormonal changes. If your migraines shift around your cycle, it is worth considering whether jaw symptoms also fluctuate at the same time.
Finally, and most practically: tell your neurologist. Even if your dentist has concluded no treatment is needed, your neurologist needs the full picture. Jaw tension as a prodrome symptom, clicking on the same side as your migraines, or TMD confirmed by a dental exam are all relevant pieces of information for someone managing your migraine treatment.
The fact that treatment may not be accessible right now due to coverage limitations does not mean the information is irrelevant. Knowing a variable exists is always better than not knowing.
FAQs
-
TMD and migraines share a bidirectional relationship through the trigeminal nerve, which is the main pain pathway for both conditions. Having one condition increases the risk of developing the other. Research suggests people with migraines are approximately six times more likely to develop TMD, and people with TMD are approximately 2.5 times more likely to experience migraines.
-
Jaw clicking on its own is not confirmed to cause migraines. Clicking without pain is common and does not always indicate significant dysfunction. That said, the underlying joint or muscle irregularity causing the clicking may contribute to jaw tension, which can act as a migraine trigger in people who are already prone to attacks.
-
The 3-finger test is an informal self-check sometimes used to assess jaw opening range. You try to place three fingers stacked vertically between your upper and lower front teeth when your mouth is open. Limited range of motion is sometimes associated with TMD, though this is not a diagnostic tool and should not replace a professional evaluation.
-
If jaw tension is contributing to your migraine, first-response options include applying heat or cold to the jaw area, consciously relaxing the jaw so your teeth are not touching, chewing gum briefly to engage and release the jaw muscles, and taking your usual migraine rescue medication. Identifying which side the tension is on can help you confirm whether this is a jaw-origin attack.
-
Research suggests it can. Studies have found that people who treat their TMD often see a reduction in migraine frequency. The relationship is bidirectional, so reducing dysfunction in one system appears to reduce the load on the shared pain pathways.
-
TMD can be associated with several connective tissue and autoimmune conditions, including rheumatoid arthritis, psoriatic arthritis, Sjogren's syndrome, systemic lupus erythematosus, and scleroderma. If you have an autoimmune diagnosis and are also experiencing jaw symptoms, it is worth raising both with your care team.
-
Yes. Even if your dentist has determined no treatment is needed right now, your neurologist should know. Jaw tension as a prodrome symptom, one-sided jaw or tooth pain on the migraine side, and a confirmed TMJ finding are all clinically relevant details for someone managing your migraine care.
The content on this page is based on personal experience and is not medical advice. Always consult your doctor regarding your migraine management and treatment plan.
QUICK ANSWER: TMJ disorder (temporomandibular disorder, or TMD) and migraines share a bidirectional relationship, meaning each condition increases the risk of the other. They share a common pain pathway through the trigeminal nerve, which is the same nerve involved in migraine attacks. Research shows that people with migraines are approximately six times more likely to develop TMD, and people with TMD are approximately 2.5 times more likely to experience migraines. TMJ disorder is not considered a direct cause of migraines, but it is recognized as a trigger.